The news that one might be suffering from a heart condition that requires a heart stent can be stressful to process. It is important to understand the reasons why your doctor might have recommended a stent in the first place.
Arteries are blood vessels that carry out the function of circulating blood away from the heart to the rest of the body. They are shaped like tubes and the pumping contractions of the heart propel the blood through the arteries.
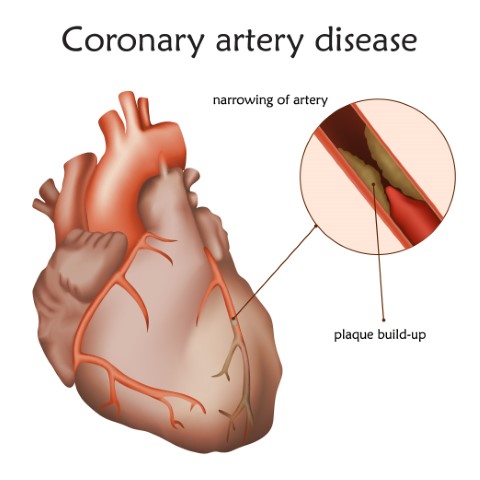
When a buildup of plaque i.e cholesterol, fat, and other substances collect in the bloodstream, it sticks to the walls of the arteries, and over time, this buildup narrows the arteries, limiting the amount of fresh blood that can be circulated to the body.
Over time, people with narrowed coronary arteries may begin to notice symptoms such as chest pain. This buildup of plaque in the coronary arteries is a cause of coronary heart disease. People with this condition may be at a higher risk of many serious complications such as a heart attack or a stroke if they do not receive treatment.
What is Coronary Artery Disease? Coronary Artery Disease (CAD) is the most common form of heart disease. It occurs when one or more of the coronary arteries becomes narrow, thus restricting the flow of blood to the heart muscle. Without adequate blood, supply the heart becomes starved of oxygen and vital nutrients required for the proper functioning of the heart muscle which may lead to chest pain called angina. The process is often called hardening of the arteries or atherosclerosis.
Symptoms of CAD may include
Early warning signs such as
- A squeezing, suffocating, or burning feeling in your chest tends to start in the center of your chest but may move to your arm, neck, back, throat or jaw.
- fatigue
- pain
- dizziness
Symptoms in women are comparatively non-traditional:
- vague chest discomfort
- fatigue
- indigestion
- Anxiety
- sleep difficulties
If left untreated, CAD can lead to other serious problems such as heart attack, stroke, or even death.
When a coronary artery is narrowed by a buildup of fatty deposits called plaque, it can reduce blood flow, causing chest pain. If a clot forms and completely blocks the blood flow to part of the heart muscle, it can result in a heart attack.
Therefore if the artery is at risk of collapsing or becoming blocked, doctors may recommend inserting a stent to keep it open.
What is a stent?
A stent is a tiny wire mesh tube that your doctor can insert into a blocked artery passageway to keep it open. Its function is to open the blocked artery and post-treatments stents remain permanently in the body. Stents are made of either metal or plastic. Stents can also be coated with medication to help keep a blocked artery from closing.
How are stents used?
The stent is mounted on a balloon catheter. It is tracked through the artery to the narrowed segment/blockage which is then moved into the area of the blockage. The balloon is then inflated resulting in the stent expanding and locking in place, forming a scaffold that holds the artery open. The balloon is then deflated and withdrawn.
The stent stays permanently and improves blood flow to the heart muscle. Stents are used based on the features of the artery blockage such as the size of the artery and where the blockage is.
What are the advantages of using a stent?
- After balloon angioplasty or other procedures that use catheters, certain patients may experience a re-narrowing of the artery. Stents help to reduce the re-narrowing.
- Patients who have angioplasty and stents have less discomfort and also recover faster from these procedures as compared to patients that choose to undergo coronary artery bypass surgery (CABG)
How long will a stent last? Are stents permanent?
Commonly used metallic stents are permanent and stay in the body for lifelong.
Re-narrowing (Restenosis) of the treated coronary artery can occur in some cases and may require a re-intervention in the future. However, with the latest generation, the drug-eluting stents’ restenosis rate has reduced significantly.
Bioresorbable scaffold or stent is the latest innovation in the field of stent technology. Unlike metallic stents, they don’t stay permanently inside the patient body. Post healing, they dissolve naturally in 2-3 years thus leaving the artery in its natural state.
What happens after stent insertion?
Depending on the insertion site, there may be soreness, for which mil painkillers are usually given. Your doctor might prescribe medication to prevent clotting, and might want you to remain at the hospital overnight. This helps ensure that there are no complications. In cases of coronary events like a heart attack or a stroke, you might be asked to stay for a longer time. Depending on the severity of the cause of the stent insertion, such as a heart attack, recovery might take a while. Until then it is advised to take it easy for a couple of weeks, avoid heavy lifting, etc.
Are there any risks involved in the insertion of stents?
Like any other medical procedure, Stenting may also involve risk, but with the latest advancement in technology and the treatment procedure, it has been minimized significantly. One should discuss and understand with their Physician about the common risk factors which is involved with stenting.
Some of the common risk factors may include bleeding from the treatment site like groin from where the catheter was introduced, allergic reaction to dye or stent, re-narrowing of the artery or clot formation, etc
Insertion of a foreign body in your blood, there is a one in 50 chance of blood clots forming on the stent. Your physician may prescribe certain medications to lower the risk of blood clots.
While a stent can result in remarkable improvement of your condition, it is not a cure for heart disease. You will need to address the contributing factors like high blood pressure, cholesterol, and being overweight as well. Eating a well-balanced diet, exercising regularly, even quitting smoking can lead to a heart-healthy lifestyle.
Disclaimer: This blog is only for awareness purposes. We do not intent to promote any medications given in the blog. Please consult your physician before taking any medication.